Luna mHealth: a Global Health Application for Resource-Constrained Communities Lacking Internet Access
This page is a high-level overview of my primary research project. Conceived of by Eliana Socha in spring 2021, we now are creating a production-quality system.
Problem description
Rural areas around the world face unique difficulties in accessing health services. Many members of rural communities in developing countries rely on home care and traditional providers, including midwives and plant medicine practitioners1. Access to health education can also be limited, with low adult literacy levels and limited access to schooling and resources for self-education2. It has been shown that providing community members with culturally relevant and contextually appropriate health education can empower them to practice preventive health and seek care when necessary3.
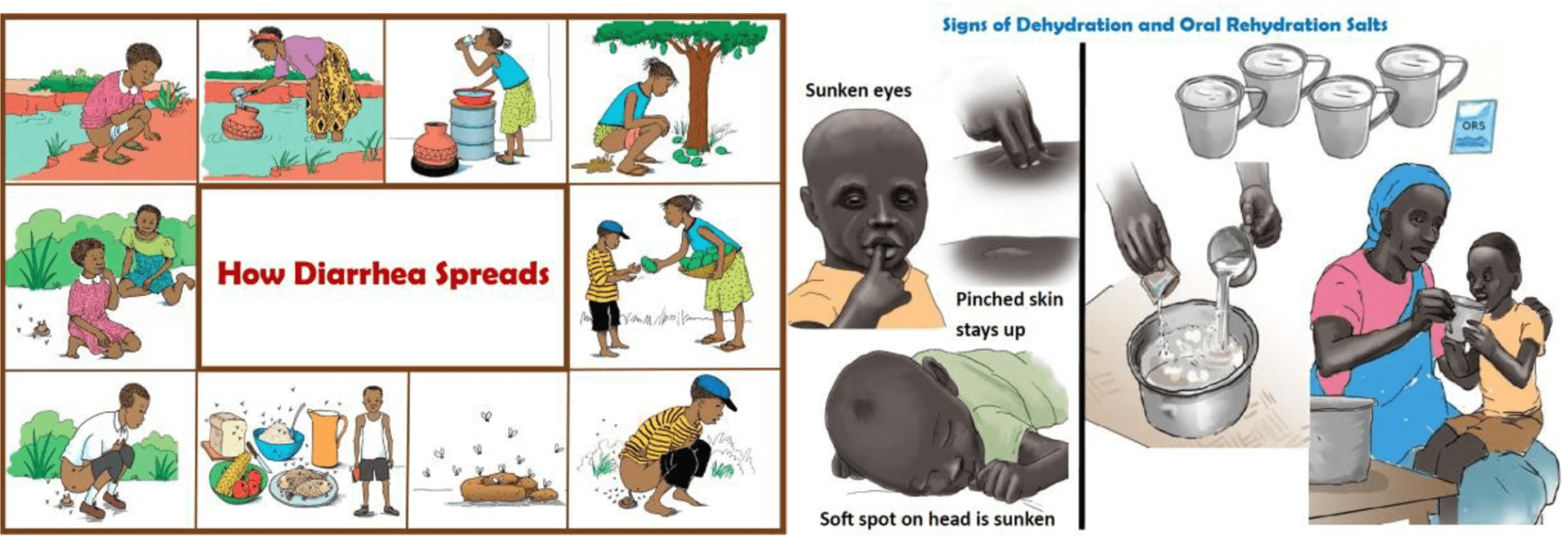
The project vision emerged from Eliana Socha’s 4 years in the Peace Corps living and working in an indigenous region of Panama, the Comarca Ngäbe-Buglé, although our goal is for the framework developed for Luna to ultimately be usable across a broad range of applications. This Comarca Ngäbe-Buglé region, the most undeveloped area of the country, faces a number of barriers to adequate healthcare access and education, including low numbers of healthcare facilities and workers, low economic access to services, and low levels of adult literacy, especially among mothers4. These barriers are reflected in poor health outcomes, including a maternal mortality rate 58 times higher than the national average and diarrhea as the leading cause of death on the reservation4.
As mobile health technology has advanced, with more sophisticated and technologically advanced solutions available to many smartphone users, areas like the Comarca have been left out. There is a need for health education tools that are comprehensive, accessible, and aimed at a rural population with low health literacy and limited access to both physical and technological services such as Internet access.
Solution concept
Our project is developing a cellphone-based framework that can reach key underserved and resource-constrained populations in global health by providing community members and workers, such as rural mothers and midwives, with a mobile app they can use for home health education on topics such as prenatal and postnatal care.
We expect that the Luna app would be used in a combined approach in the Comarca Ngäbe-Buglé, with midwives or healthcare workers first using it as a guided, interactive teaching tool and then passing it to community members’ phones for further review and self-education at home.
The app design includes a number of features to make it accessible in low-resource settings: free; audio-visual content for non-literate populations; offline use for areas with no cell coverage or Internet access; materials available in various languages.
In tandem with the mobile app we are developing an authoring system to allow healthcare professionals and organizations to create content modules via Microsoft PowerPoint or the freely available LibreOffice Impress. The authoring system will support translating the written text into multiple written languages, and recording the text as spoken-word audio files in multiple languages. This will allow readers to read or listen to the text in the language of their choice.
Authors may use built-in interactive pages to help readers practice recall about things like which foods provide which benefits, definitions of key terms, or what activities must precede other activities.
The authoring system will package all of these into a content module that readers may read share with each other via BlueTooth without needing Internet access.
Reduction to practice
We have completed a proof-of-concept and now are building a deployable app and authoring system.
The initial content modules for field testing will focus on key problems in global maternal and infant health, with modules that teach preventive health and help people recognize symptoms that may need urgent medical attention. We are beginning with a module on pre- and post-partum health, nutrition, and danger signs, as this is especially relevant in the region. We are basing the content design on the principle that people are most empowered to take control of their health when they are given tools to self-educate.
The educational techniques and materials for the initial use case that will be adapted for digital use in the app have been developed and tested in the field by the project team. Ms. Socha has designed and managed women’s health education programs in Brazil, South Sudan, and Panama, with Peace Corps and Médecins Sans Frontières; the modules will digitally adapt the participatory educational techniques that she has tested and honed in rural communities.
The material for the Comarca Ngäbe-Buglé will be developed to be culturally and contextually relevant, drawing on user-testing and Eliana Socha’s Peace Corps experience of 4 years working in women’s health in the region.
Pathway to implementation
We have a multi-phase plan for implementation whose actual path will depend upon the community partners we work with. We plan to start locally, working with partner organizations near the development team in Seattle, WA and then expand to partners that work with communities in Panama, Guatemala, or elsewhere. At each step, we plan to do field testing to better understand the context of opportunity and iteratively improve the system. We aim to have a pilot version developed and ready for field testing in 2024.
After the pilots, we will offer the app as a free and open-source and easily accessible tool for organizations that work with relevant populations, including but not limited to healthcare applications in rural areas. We are envisioning both a broad implementation, for organizations to use the tool as best suits their needs, and a targeted implementation to areas with the following characteristics: rural populations, low healthcare access, high rates of illiteracy, and growing access to cell phones.
This will allow Luna to scale its usage in scope, by allowing other experts to add more content modules or adapt existing modules, and in range, by adapting the material for different languages and cultural contexts.
References
- Davy C, Harfield S, McArthur A, et al. Access to primary health care services for Indigenous peoples: A framework synthesis. Int J Equity Health. 2016 Sep 30; 15(163). Available from: https://doi.org/10.1186/s12939-016-0450-5
- Madeeha M, Rubab Z Z, Azhar H. Health Literacy as a Global Public Health Concern: A Systematic Review. J of Pharmacol & Clin Res. 2017 Nov 13; 4(2): 555632. Available from: 10.19080/JPCR.2017.04.555632
- Goel S, Bhatnagar N, Sharma D, Singh A. Bridging the Human Resource Gap in Primary Health Care Delivery Systems of Developing Countries With mHealth: Narrative Literature Review. JMIR Mhealth Uhealth. 2013 Dec 3;1(2):e25. Available from: 10.2196/mhealth.2688
- República de Panamá. (2010-2020). Instituto Nacional de Estadística y Censo [Data file]. Retrieved from https://www.inec.gob.pa/publicaciones/Default.aspx
Project history
| Spring 2021 | Eliana Socha conceives of project |
| Winter 2022 | Jon Socha creates initial content module structure |
| Spring 2023 | Kishan Negendra* demonstrates prototype system |
| Autumn 2024 | Ashish Nagar*, Mykyta Skiba*, Shaun Stangler* start building production-quality system |
| Winter 2024 | Alan Lai*, Bruce Butterfield join project |
| Spring 2024 | Akshay Gopalakrishnan*, Wonwhoo (Andrew) Nah*, Joel Aguiar*, Olivia Munineath Borath*, Vanshika Singh* join project
Prof Mabel Ezeonwu begins collaborating on recruiting and engaging communities for field testing and use |
*UW Bothell student under my supervision